|
713-465-0696 Houston, Texas |
Arthroscopic Anterior Cruciate Ligament Reconstruction - The State Of The ArtClick here to view actual ACL surgery
INTRODUCTION:

Orthopedists estimate that only about twenty percent of people who tear their anterior cruciate ligament and do not have surgical treatment do well over the years. Eighty percent of the people who tear their anterior cruciate ligament and who leave it untreated will develop significant secondary problems with their knee requiring various surgical procedures. Secondary problems include the development of torn cartilages, loose bodies, arthritis, or a painful knee. Women tend to do worse following an anterior cruciate ligament injury than do men. If an individual is very active and wishes to continue playing vigorous sports and other high demand activities, then anterior cruciate ligament reconstruction should be performed to restore knee stability. If one feels that his or her athletic career is near its end and they have become less active, then anterior cruciate surgery is not required. I do not recommend continuing to play sports on an unstable knee as it has been shown repeatedly that the knee will go on to develop multiple problems as a result of the instability. Arthroscopic anterior cruciate reconstruction is a major advancement in the treatment of an acute or chronic tear of the anterior cruciate ligament. Since 1987, arthroscopic technology has advanced to allow for ligament reconstruction of the knee without cutting the knee open. I was one of the first orthopedists in Houston to perform this type of procedure, and since 1987 I have performed over 1200 of these procedures. Here are its benefits: At the time of surgery prior to reconstruction of the ligament, a complete diagnostic arthroscopy of the knee is performed. All other damage including torn cartilages, bone chips, or any other problem within the knee is repaired prior to ligament reconstruction.  Through the use of arthroscopy, a new anterior cruciate ligament can be made for the knee and be placed within the knee joint without making a large cut on the knee. A one-inch incision and three arthroscopy cuts are used to perform this operation. The procedure, as I have developed it, allows me to make small, pleasing cosmetic incisions. Drill holes are placed within the bone and the new ligament is held in place with dissolving screws. The surgeon and patient have a choice of the material used to reconstruct the anterior cruciate ligament. Most of the time, I perform a hamstring graft with the semitendinosus and gracilis tendon from the patient. Occasionally, a cadaver allograft (donor tissue) of the patellar tendon or of hamstring tendon may be utilized for various reasons. The patient has the option of requesting a cadaver graft. The success rate of this surgery is over ninety-give percent. Rehabilitation may be started immediately. The arthroscopic technique for anterior cruciate ligament reconstruction allows this procedure to be performed as an outpatient procedure. The patient may start riding a stationary bicycle or use a StairMaster less than one week following the surgery. Walking with weight bearing and the use of crutches is started immediately following the surgery. Gradually the patient adjusts to one crutch, and then is crutch free, as tolerated. Some individuals go to physical therapy after surgery; others do their own therapy. While it is not mandatory to go to a physical therapist, it is mandatory to exercise the knee regularly for a significant period of time following the procedure. It generally takes six to nice months to fully rehabilitate the knee following this surgery. High velocity contact sports such as football, basketball, volleyball, or downhill skiing are usually allowed at six to nine months following the surgery. This delay in time gives the new ligament a chance to develop a new blood supply and become strong. It is generally recommended that the patient wait two to four weeks following the initial injury of the knee before anterior cruciate ligament reconstruction is performed. The reason for delaying surgery at least two weeks is to allow the soreness of the knee joint to go away and to allow the person to recover to a full range of motion before surgery is undertaken. It has been shown that this waiting period makes rehabilitation from the surgery much easier and the results better. Additionally, I recommend the use of a continuous passive motion machine (CPM) immediately following the surgery to recover range of motion to the knee. Most insurance companies cover the cost of home rental of the CPM. If not, it can be rented through a medical equipment company. I recommend Therapeutic Solutions at 281-922-5453. In addition, to obtain full bending of the knee with the CPM machine, the post operative patient must work especially hard to regain full extension of the knee. If full range of motion of the knee is achieved, the result of this type of surgery is excellent. If there are any questions, I will be happy to answer them. Contact me by clicking here to send me a message or call me at 713-465-0696. Larry L. Likover, M.D., P.A. |
  |
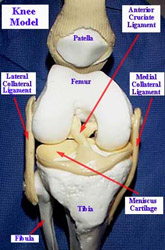 A tear of the anterior cruciate ligament is the most common major ligamentous tear of the knee. Initially, the injured person develops a swollen painful knee because the ligament bleeds when it tears and fills the knee with blood. Over a period of time, the blood disappears and the pain diminishes; the knee, however, remains unstable. The anterior cruciate ligament is a very important knee ligament for stability of the knee. It is basically a "cable" or "rope" and a tear of this ligament usually causes significant instability of the knee. This instability can severely affect the future function of the knee joint for sports requiring changing of direction and work activities requiring lifting, climbing and straining. Once the knee becomes unstable as a result of ligamentous injury, the knee joint is much more prone to further injury, such as tearing one or both of the cartilages (menisci) and the development of loose bodies or arthritis over a period of time. Overall, the knee has a tendency to deteriorate significantly if it remains unstable and the initial ligament injury is not treated properly.
A tear of the anterior cruciate ligament is the most common major ligamentous tear of the knee. Initially, the injured person develops a swollen painful knee because the ligament bleeds when it tears and fills the knee with blood. Over a period of time, the blood disappears and the pain diminishes; the knee, however, remains unstable. The anterior cruciate ligament is a very important knee ligament for stability of the knee. It is basically a "cable" or "rope" and a tear of this ligament usually causes significant instability of the knee. This instability can severely affect the future function of the knee joint for sports requiring changing of direction and work activities requiring lifting, climbing and straining. Once the knee becomes unstable as a result of ligamentous injury, the knee joint is much more prone to further injury, such as tearing one or both of the cartilages (menisci) and the development of loose bodies or arthritis over a period of time. Overall, the knee has a tendency to deteriorate significantly if it remains unstable and the initial ligament injury is not treated properly.